Glomerulonephritis is a class of diseases caused by the inflammatory process of the microscopic structural elements of the kidneys called glomeruli, which have the function of filtering the blood and remove waste products. When the glomeruli are inflamed, the functions become ineffective, causing proteinuria, hematuria, edema, and risking chronic kidney disease and end-stage renal disease. Acute or chronic GN; possible causes of it are infectious, autoimmune diseases, genetic conditions, and environmental exposures.
Pathophysiology of Glomerulonephritis
Glomerulonephritis: Glomerulonephritis starts when the immune system mistakenly attacks the glomeruli, resulting in inflammation and scarring. There are several different types of GN, each with a distinct pathophysiology.
Post-infectious GN: It is often found after infections such as streptococcal pharyngitis. The immune system produces complexes in an effort to clear the infection but these immune complexes get trapped within the glomeruli, leading to an inflammatory reaction.
IgA Nephropathy, also known as Berger's Disease, is the most common form of primary GN. It presents with episodes of hematuria due to the deposition of IgA antibodies in the glomeruli.
Membranous Nephropathy This presents with a thickening of the glomerular basement membrane due to immune complex deposition and is often associated with other autoimmune diseases like lupus.
Focal Segmental Glomerulosclerosis (FSGS): Scarring within a few areas of the glomeruli, possibly caused by viral infections, genetic mutations, or drug toxicity.
Lupus Nephritis: A form of secondary GN that occurs in patients with systemic lupus erythematosus (SLE), where autoantibodies target and damage the kidneys.
This latter mechanism disrupts the filtering mechanism of the kidney and thus leaks proteins and red blood cells into the urine. Prolonged injury may eventually lead to glomerular sclerosis, loss of renal function, and progression to CKD.
| Mechanism of Action | Key Drugs/Technologies | Companies/Organizations Involved |
|
Complement Inhibition |
Eculizumab (Soliris) |
Alexion Pharmaceuticals (AstraZeneca) |
|
Endothelin Receptor Antagonism |
Sparsentan |
Travere Therapeutics |
|
T-Cell Modulation (Calcineurin Inhibition) |
Voclosporin |
Aurinia Pharmaceuticals |
|
Anti-Fibrotic Therapy |
Bardoxolone methyl |
Reata Pharmaceuticals |
|
B-cell Inhibition (Monoclonal Antibodies) |
Obinutuzumab, Rituximab (in new trials) |
Genentech (Roche), Novartis |
|
Oxidative Stress Modulation |
Bardoxolone methyl |
Reata Pharmaceuticals |
|
ANCA-Associated Vasculitis Treatment |
Avacopan (Tavneos) |
ChemoCentryx (Amgen) |
|
B-cell Activation Inhibition |
Belimumab |
GlaxoSmithKline (GSK) |
Epidemiology and Risk Factors
Glomerulonephritis is a disease that affects everyone on the planet, and incidence and prevalence differ with the type of GN and region. Post-infectious GN and IgA nephropathy are more common in developing countries, while conditions like FSGS and lupus nephritis are more typical in Western populations.
| Type of GN | Prevalence/Incidence |
|---|---|
|
IgA Nephropathy |
Most common globally, affecting ~25-50 per million |
|
Post-Infectious GN |
Higher incidence in developing countries due to infection rates |
|
FSGS |
Rising incidence, particularly in African Americans |
|
Membranous Nephropathy |
Second most common cause of nephrotic syndrome in adults |
Various risk factors have been associated with the development of GN:
Infections: The risk of developing post-infectious GN or membranoproliferative GN increases with viral and bacterial infections (e.g., streptococcus, hepatitis B, hepatitis C, HIV).
Autoimmune diseases: SLE and ANCA-associated vasculitis can cause glomerulonephritis.
Genetics: There are specific genetic mutations that predispose individuals to diseases such as FSGS.
Ethnicity: In FSGS, African Americans appear to be overrepresented and are more likely to present with poor outcomes. This is partly due to genetic predispositions, such as mutations of the APOL1 gene.
Symptoms and Diagnosis
The symptoms of glomerulonephritis vary with the causative factor and the severity of the disease as follows:
Proteinuria: The presence of excessive proteins in the urine, which makes it frothy.
Hematuria: The presence of blood in the urine, which makes it pink or cola-colored
Edema: Drooping around the face, hands, feet, and abdomen due to fluid retention
Hypertension: High blood pressure caused by a failing kidney.
Decreased urine volume: It represents poorly working kidneys.
The diagnosis of GN typically includes:
Urinalysis: to determine the presence of proteinuria, hematuria, and other urinary abnormalities
Blood tests: the patient's renal function may be assessed through laboratory studies such as creatinine and GFR, and immune markers such as complement levels and ANCA antibodies
Renal biopsy: A tissue biopsy is often necessary to confirm the diagnosis, as it can be established that there is damage to the glomeruli and what kind of GN
Imaging of the kidneys: Ultrasound and MRI are used to assess the size and structure of the kidneys.
Treatment of Glomerulonephritis
The treatment of glomerulonephritis depends on the cause of the disease, the type of GN, and the severity of the disease. Important treatment approaches are:
1. Immunosuppressive Therapy
Corticosteroids: Corticosteroids, such as prednisone, are one of the most widely used treatments that exert immunosuppressive effects to reduce inflammation in conditions like IgA nephropathy, lupus nephritis, and FSGS.
2. Cyclophosphamide and mycophenolate mofetil (CellCept)
These are used in more severe or refractory cases, mainly in autoimmune-related GN like lupus nephritis and ANCA-associated vasculitis.
Rituximab: A monoclonal antibody directed against B-cells, utilized in autoimmune glomerulonephritis of lupus nephritis and ANCA vasculitis.
3. RAAS Inhibitors
ACE inhibitors, like lisinopril, and angiotensin receptor blockers (ARBs), like losartan, are important measures in reducing proteinuria and controlling blood pressure to slow the disease process.
3. Plasmapheresis
Used in rapidly progressive GN or cases associated with ANCA vasculitis, plasmapheresis removes circulating antibodies and immune complexes that contribute to the inflammation of the glomeruli.
4. Supportive Care
Diuretics for controlling edema, antihypertensive agents, and alterations in diet (for instance, low sodium and low protein) are often necessary to control symptoms and promote slowing of renal damage.
Emerging Therapies and Clinical Trials
Emerging therapies in GN involve the participation of particular immune pathways and decreased use of chronically used corticosteroids and other broad immunosuppressants. Present studies entail:
1. Complement Inhibition:
The most significant role of the complement system was activation as a hallmark of tissue injury in diseases such as membranoproliferative GN and atypical hemolytic uremic syndrome (aHUS). A complement inhibitor eculizumab is under investigation that lowers damage caused by the complements.
2. Monoclonal Antibodies:
Rituximab, being effective at depleting B-cell activities and which has demonstrated some effectiveness in the treatment of lupus nephritis and ANCA vasculitis, is under investigation in a more varied group of GN types.
Other B-cell inhibitors being pursued include belimumab, an agent potentially applicable to the treatment of lupus nephritis.
3. B Cell and T Cell Modulation:
Targeted therapies such as cyclosporine, a calcineurin inhibitor, are under development for lupus nephritis aimed to suppress the activation of T cells and subsequent inflammation without the adverse effects usually incurred with the use of standard immunosuppressants.
4. Anti-Fibrotic Therapies:
Pirfenidone and bardoxolone methyl, which were initially created for pulmonary fibrosis, are now being put to the test for the purpose of slowing kidney fibrosis and the progression of GN.
5. Gene Therapy:
Genetic forms of GN, including FSGS, have therefore become targets for gene therapy approaches to correct the very mutations that give rise to the disease. Such an approach is very useful for a patient with APOL1 gene mutations.
Patient Demographics and Risk Stratification
The condition occurs in all age groups, but there are certain demographic factors that influence the prevalence and severity of the condition.
Any age: GN can occur at any age, whereas other conditions like IgA nephropathy are often present in young adults while lupus nephritis typically occurs in women of childbearing age.
Gender: Autoimmune-associated GN, like lupus nephritis, is predominantly found among women, but FSGS is predominantly seen in men.
Ethnicity: African Americans have a high incidence of FSGS and high ESRD rates due to GN, compared to the majority of other racial groups, probably due to genetic factors like APOL1 mutations.
Future Directions and Challenges
The development of GN treatment in the future is primarily aiming at the establishment of therapies that can target specific immune mechanisms, with less dependence on broad immunosuppressants like corticosteroids, having very severe adverse effects.
1. Precision Medicine:
Advances in genetic testing and biomarker discovery are likely to allow clinicians to make treatment tailored to the cause of GN. For instance, the discovery of certain genetic mutations like APOL1 in FSGS patients can give clinicians the appropriate targeted therapy to apply.
2. Global Access and Disparities in Care:
Access to early diagnosis and treatment is practically absent in most low- and middle-income countries. New therapies available, like monoclonal antibodies and complement inhibitors, need to be made available and accessible to reduce the burden of GN worldwide.
3. Long-term Management and Kidney Transplantation:
Patients with progressive GN are at high risk for progression to CKD and may eventually have end-stage renal disease with the need for dialysis or kidney transplantation. Emerging research in areas of regenerative medicine and the prevention of injury to the kidneys are critical to enhancing the long-term outlook for such patients.
Table of Contents (ToC) for Nephrotic Syndrome
1.1 Definition and Overview
1.2 Epidemiology and Prevalence
1.3 Types of Nephrotic Syndrome (Primary vs. Secondary)
2.1 Mechanisms of Glomerular Injury
2.2 Role of Podocyte Damage and Proteinuria
2.3 Underlying Causes: Minimal Change Disease, Focal Segmental Glomerulosclerosis (FSGS), and Membranous Nephropathy
3.1 Key Symptoms: Proteinuria, Hypoalbuminemia, Edema, and Hyperlipidemia
3.2 Complications: Thrombosis, Infections, and Acute Kidney Injury
3.3 Impact on Quality of Life and Long-Term Health
4.1 Urinalysis and Proteinuria Measurement
4.2 Blood Tests: Serum Albumin, Lipid Profile, and Renal Function
4.3 Renal Biopsy and Histopathological Findings
5.1 Corticosteroids and Immunosuppressive Therapies
5.2 Management of Edema: Diuretics and Salt Restriction
5.3 Anticoagulation for Thrombotic Risk
5.4 Lipid-Lowering Agents and Managing Hyperlipidemia
6.1 New Immunomodulatory Drugs (Rituximab, Tacrolimus, Cyclophosphamide)
6.2 Biological Therapies Targeting Podocyte Protection
6.3 Investigational Therapies for FSGS and Membranous Nephropathy
6.4 Stem Cell Research and Regenerative Medicine in Nephrotic Syndrome
7.1 Preventing and Managing Relapse
7.2 Monitoring for Chronic Kidney Disease (CKD) Progression
7.3 Managing Complications: Hypertension, Infection, and Osteoporosis
8.1 Dietary Changes and Sodium Restriction
8.2 Monitoring Fluid Balance and Weight
8.3 Patient Education and Psychological Support
9.1 Risk Factors for Disease Relapse and Progression
9.2 Long-Term Kidney Function and Risk of End-Stage Renal Disease (ESRD)
9.3 Impact on Growth and Development in Pediatric Nephrotic Syndrome
10.1 Advances in Personalized Medicine for Nephrotic Syndrome
10.2 Addressing the Genetic and Molecular Basis of the Disease
10.3 Improving Outcomes and Reducing Relapse Rates
An accurate research report requires proper strategizing as well as implementation. There are multiple factors involved in the completion of good and accurate research report and selecting the best methodology to compete the research is the toughest part. Since the research reports we provide play a crucial role in any company’s decision-making process, therefore we at SNS Insider always believe that we should choose the best method which gives us results closer to reality. This allows us to reach at a stage wherein we can provide our clients best and accurate investment to output ratio.
Each report that we prepare takes a timeframe of 350-400 business hours for production. Starting from the selection of titles through a couple of in-depth brain storming session to the final QC process before uploading our titles on our website we dedicate around 350 working hours. The titles are selected based on their current market cap and the foreseen CAGR and growth.
The 5 steps process:
Step 1: Secondary Research:
Secondary Research or Desk Research is as the name suggests is a research process wherein, we collect data through the readily available information. In this process we use various paid and unpaid databases which our team has access to and gather data through the same. This includes examining of listed companies’ annual reports, Journals, SEC filling etc. Apart from this our team has access to various associations across the globe across different industries. Lastly, we have exchange relationships with various university as well as individual libraries.

Step 2: Primary Research
When we talk about primary research, it is a type of study in which the researchers collect relevant data samples directly, rather than relying on previously collected data. This type of research is focused on gaining content specific facts that can be sued to solve specific problems. Since the collected data is fresh and first hand therefore it makes the study more accurate and genuine.
We at SNS Insider have divided Primary Research into 2 parts.
Part 1 wherein we interview the KOLs of major players as well as the upcoming ones across various geographic regions. This allows us to have their view over the market scenario and acts as an important tool to come closer to the accurate market numbers. As many as 45 paid and unpaid primary interviews are taken from both the demand and supply side of the industry to make sure we land at an accurate judgement and analysis of the market.
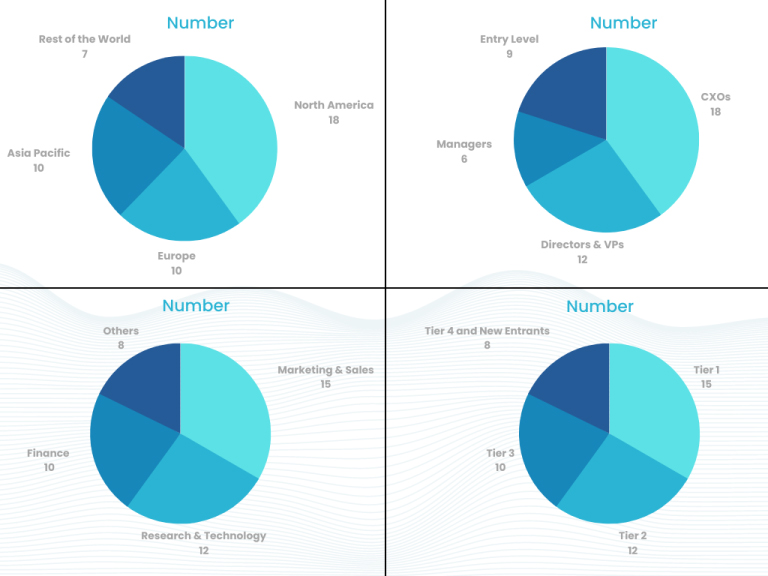
This step involves the triangulation of data wherein our team analyses the interview transcripts, online survey responses and observation of on filed participants. The below mentioned chart should give a better understanding of the part 1 of the primary interview.
Part 2: In this part of primary research the data collected via secondary research and the part 1 of the primary research is validated with the interviews from individual consultants and subject matter experts.
Consultants are those set of people who have at least 12 years of experience and expertise within the industry whereas Subject Matter Experts are those with at least 15 years of experience behind their back within the same space. The data with the help of two main processes i.e., FGDs (Focused Group Discussions) and IDs (Individual Discussions). This gives us a 3rd party nonbiased primary view of the market scenario making it a more dependable one while collation of the data pointers.
Step 3: Data Bank Validation
Once all the information is collected via primary and secondary sources, we run that information for data validation. At our intelligence centre our research heads track a lot of information related to the market which includes the quarterly reports, the daily stock prices, and other relevant information. Our data bank server gets updated every fortnight and that is how the information which we collected using our primary and secondary information is revalidated in real time.

Step 4: QA/QC Process
After all the data collection and validation our team does a final level of quality check and quality assurance to get rid of any unwanted or undesired mistakes. This might include but not limited to getting rid of the any typos, duplication of numbers or missing of any important information. The people involved in this process include technical content writers, research heads and graphics people. Once this process is completed the title gets uploader on our platform for our clients to read it.
Step 5: Final QC/QA Process:
This is the last process and comes when the client has ordered the study. In this process a final QA/QC is done before the study is emailed to the client. Since we believe in giving our clients a good experience of our research studies, therefore, to make sure that we do not lack at our end in any way humanly possible we do a final round of quality check and then dispatch the study to the client.
Hi! Click one of our member below to chat on Phone
© 2025 All Rights Reserved by SNS Insider Pvt Ltd