CF is an autosomal, recessive inherited disorder that has a presence in approximately 70,000 people around the world. It causes mutations in the CFTR gene where the dysfunctional transport of chloride and bicarbonate ions takes place. This subsequently increases the mucus trap at various points, mainly through the respiratory and gastrointestinal tract. This gives way to frequent infections, inflammation, and final deterioration of lung function. Over the past two years, however, treatment for CF has dramatically changed with the discovery of CFTR modulators and even gene therapy.
1. CFTR Modulators: CFTR modulators changed the whole strategy to treat cystic fibrosis because they actually fix the disease's root cause, the CFTR protein. Ivacaftor, lumacaftor, and a triple combination (elexacaftor/tezacaftor/ivacaftor, Trikafta) improve CFTR protein function based on the mutation chosen. Lung function and quality of life are now appreciably improved with these drugs, which the authors consider disease-modifying for patients with eligible mutations, which is over 90% of the CF population.
2. Gene Therapy: Gene editing technologies, such as CRISPR-Cas9, could lead to a point where completely curative treatments for CF are on the horizon. Gene replacement therapy would involve replacing functional CFTR genes within affected cells, thus providing a long-term basis for treating patients with CF. Scientists are currently working on inhaled gene therapy delivery that would directly administer corrective genetic material to the lung.
3. Anti-infective therapies: Chronic infection of the lung is one of the most important reasons for morbidity associated with CF. New generations of antibiotics and anti-infective therapy strategies, including inhaled antimicrobials and new combination regimens, are under investigation for managing recalcitrant infections, particularly by Pseudomonas aeruginosa.
| Mechanism of Action | Key Drugs/Technologies |
|---|---|
|
CFTR Modulation |
Ivacaftor, Lumacaftor, Tezacaftor, Elexacaftor |
|
Gene Therapy |
CRISPR-Cas9, Inhaled Gene Therapy |
|
Anti-infective Therapies |
Inhaled antibiotics, Novel antimicrobial agents |
Expanded Patient Population and Epidemiology
The most prevalent fatal genetic disorder leading to it is cystic fibrosis, with an estimated 70,000 cases worldwide and approximately 40,000 in the U.S. The disorder arises because of mutations in the CFTR gene, which thereafter affects chloride channel function and results in the formation of thick, sticky mucus in the lungs, pancreas, and other organs.
Global Prevalence and Genetic Variability
Incidence: The incidence of CF is most predominant in Caucasians of European origins. However, the incidence is within an average of 1:2,500 to 1:3,500 neonates. It has also been found to be less common in populations other than Caucasians such as African Americans, Asians, and Hispanics, and the incidence rate could be as low as 1 in 15,000-20,000.
CF is also less diagnosed in many parts of Africa and Asia due to lack of awareness, and newborn screening, and it is challenging to diagnose.
Neonatal screening programs have immensely raised the early case detection rate in most developed countries and have improved life expectancy. Newborn screening for cystic fibrosis has been instituted as a routine investigation in the United States, Europe, and Canada. Thus, the diagnoses have been made earlier, and interventions have begun in much earlier stages for better outcomes. In LMICs, owing to the absence of neonatal screening, the diagnosis is delayed, and because most patients present much later, there is a loss of life expectancy since most of them present during severe complications.
Death and Life Expectancy
CF is no longer a disease in children that is fatal; instead, it was given a new leash of life and has increased life expectancy so much that in the USA and other developed countries, the median life expectancy for someone with CF has gone up to about 47 years due to CFTR modulator therapies and comprehensive care.
But inequities in access to more advanced treatments mean that patients from LMICs might still experience life expectancies that are dramatically reduced, often dying of the disease in their 20s and 30s.
Racial and Geographic Inequities
Although CF is less common among people of non-Caucasian ethnicity, ethnic minorities in developed countries are most exposed to worse outcomes because of both unequal access to treatment and poor-quality care. For instance, African American and Hispanic patients in the USA have even worse lung function and higher mortality rates because of limited access to CFTR modulators and specialized CF care centers.
Redress of all these disparities would contribute importantly to achieving better health outcomes for patients with CF, particularly across different demographic groups.
Expansion of CFTR Modulators
This expansion would have an important implication for future research and market impact in relation to the existing treatment options available for CF.
The introduction of CFTR modulator therapies corrects the fundamental dysfunction of the CFTR protein, and the very face of CF treatment has changed dramatically for the majority of patients. One of the most important treatments discovered so far addressed the most common CFTR mutation, F508del, that affects around 90% of CF patients. It can improve lung function substantially, reduce pulmonary exacerbations and in general create a better quality of life for the patients.
However, this would still leave a challenge in dealing with the remaining 10% of patients who harbor rare or nonsense mutations not responsive to the current modulators. This put a focus on next-generation modulator development and an expansion of genetic testing for identifying other potential therapeutic targets.
Gene Therapy and Gene Editing
Gene therapy and gene editing with CRISPR-Cas9 are some of the most exciting areas that would be looked into in the future. Such therapy may very well be curative by correction or replacement of defective CFTR genes targeting the very root of the problem. Inhaled gene therapies deliver corrective genetic material directly to the lungs, and research and development in this area are being pursued promisingly.
Trials on clinical gene editing are still in their infancy, but so far, preliminary results indicate that CRISPR-Cas9 could successfully repair CFTR mutations in vitro. The next challenge would be to bring preclinical trials into safe, effective clinical applications; hope lies in probably eliminating the lifelong medication dependence
Anti-Infective and Anti-Inflammatory Therapies
Chronic lung infections, now chiefly due to Pseudomonas aeruginosa, continue to be a major cause of morbidity and mortality in CF patients. The continuing use of new inhaled antibiotics, including liposomal amikacin, and novel combination antibiotics, is targeting resistant strains of bacteria in most cases. Other anti-inflammatory therapies are being investigated to decrease the chronic lung inflammation that typifies CF and may slow the further progression of the disease.
Market Growth and Access
Sure, the market for CF treatments is going to expand significantly with the success of CFTR modulators and gene therapies being developed. However, the cost of such treatments remains a challenge. A patient in the United States will require Trikafta costing $311,000 a year. This drug is beyond the economic reach of most people in LMICs and also among the uninsured populations
For this to happen, the availability of biosimilars together with approaches that aim to lower the cost of treatment, will play a crucial role. There are growing pressures on health organizations and pharmaceutical firms to collaborate towards making these life-saving drugs accessible worldwide. Similarly, organizations, such as the Cystic Fibrosis Foundation, are conducting further clinical trials and funding research into treatments for CF, aiming at the development of CF treatments to be accessible across the globe.
Effect of Genetic Testing and Newborn Screening
Newborn screening programs and genetic testing have increased with early diagnosis of CF, and thus better results derive from earlier treatment. In regions where these programs are more widespread, earlier treatment and lesser progression of the disease should be anticipated to occur, most especially in countries that frequently underdiagnose CF.
This, however, is only derived fully with the development of the needed infrastructure in LMICs to ensure newborns identified with CF can have their needed care and treatments.
Table of Contents:
1.1 Overview of Cystic Fibrosis
1.2 Importance of Clinical Trials in CF Treatment
1.3 Evolution of CF Treatment Landscape
2.1 Global Incidence and Prevalence
2.2 Genetic Variability and Risk Factors
2.3 Mortality and Morbidity Statistics by Region
3.1 CFTR Modulators and Precision Medicine
3.2 Gene Therapy: Emerging Hope for a Cure
3.3 Anti-infective Therapies and Management of Lung Infections
4.1 CFTR Modulation and Protein Restoration
4.2 Genetic Approaches: CRISPR and Gene Replacement
4.3 Managing Infections and Lung Damage
5.1 Advances in CFTR Modulators
5.2 Progress in Gene Therapy Trials
5.3 Novel Anti-infective Treatments in Development
6.1 Global Disparities in CF Care
6.2 Treatment Response by Genetic Mutation
6.3 Age and Gender Differences in CF Outcomes
7.1 Expansion of CFTR Modulator Coverage
7.2 Gene Therapy: Challenges and Opportunities
7.3 Market Growth and Accessibility Concerns
8.1 Summary of Key Findings
8.2 Future Directions in CF Research and Treatment
An accurate research report requires proper strategizing as well as implementation. There are multiple factors involved in the completion of good and accurate research report and selecting the best methodology to compete the research is the toughest part. Since the research reports we provide play a crucial role in any company’s decision-making process, therefore we at SNS Insider always believe that we should choose the best method which gives us results closer to reality. This allows us to reach at a stage wherein we can provide our clients best and accurate investment to output ratio.
Each report that we prepare takes a timeframe of 350-400 business hours for production. Starting from the selection of titles through a couple of in-depth brain storming session to the final QC process before uploading our titles on our website we dedicate around 350 working hours. The titles are selected based on their current market cap and the foreseen CAGR and growth.
The 5 steps process:
Step 1: Secondary Research:
Secondary Research or Desk Research is as the name suggests is a research process wherein, we collect data through the readily available information. In this process we use various paid and unpaid databases which our team has access to and gather data through the same. This includes examining of listed companies’ annual reports, Journals, SEC filling etc. Apart from this our team has access to various associations across the globe across different industries. Lastly, we have exchange relationships with various university as well as individual libraries.

Step 2: Primary Research
When we talk about primary research, it is a type of study in which the researchers collect relevant data samples directly, rather than relying on previously collected data. This type of research is focused on gaining content specific facts that can be sued to solve specific problems. Since the collected data is fresh and first hand therefore it makes the study more accurate and genuine.
We at SNS Insider have divided Primary Research into 2 parts.
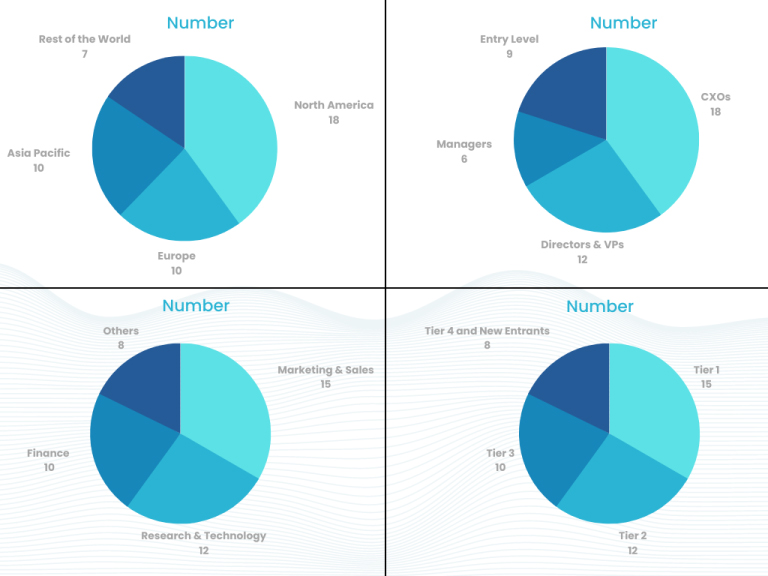
Part 1 wherein we interview the KOLs of major players as well as the upcoming ones across various geographic regions. This allows us to have their view over the market scenario and acts as an important tool to come closer to the accurate market numbers. As many as 45 paid and unpaid primary interviews are taken from both the demand and supply side of the industry to make sure we land at an accurate judgement and analysis of the market.
This step involves the triangulation of data wherein our team analyses the interview transcripts, online survey responses and observation of on filed participants. The below mentioned chart should give a better understanding of the part 1 of the primary interview.
Part 2: In this part of primary research the data collected via secondary research and the part 1 of the primary research is validated with the interviews from individual consultants and subject matter experts.
Consultants are those set of people who have at least 12 years of experience and expertise within the industry whereas Subject Matter Experts are those with at least 15 years of experience behind their back within the same space. The data with the help of two main processes i.e., FGDs (Focused Group Discussions) and IDs (Individual Discussions). This gives us a 3rd party nonbiased primary view of the market scenario making it a more dependable one while collation of the data pointers.
Step 3: Data Bank Validation
Once all the information is collected via primary and secondary sources, we run that information for data validation. At our intelligence centre our research heads track a lot of information related to the market which includes the quarterly reports, the daily stock prices, and other relevant information. Our data bank server gets updated every fortnight and that is how the information which we collected using our primary and secondary information is revalidated in real time.

Step 4: QA/QC Process
After all the data collection and validation our team does a final level of quality check and quality assurance to get rid of any unwanted or undesired mistakes. This might include but not limited to getting rid of the any typos, duplication of numbers or missing of any important information. The people involved in this process include technical content writers, research heads and graphics people. Once this process is completed the title gets uploader on our platform for our clients to read it.
Step 5: Final QC/QA Process:
This is the last process and comes when the client has ordered the study. In this process a final QA/QC is done before the study is emailed to the client. Since we believe in giving our clients a good experience of our research studies, therefore, to make sure that we do not lack at our end in any way humanly possible we do a final round of quality check and then dispatch the study to the client.
Hi! Click one of our member below to chat on Phone
© 2025 All Rights Reserved by SNS Insider Pvt Ltd